
VDRL TEST
Venereal Disease Research Laboratory (VDRL) Test is a slide flocculation test employed in the diagnosis of
syphilis. Since the antigen used in this test is cardiolipin, which is a lipoidal extracted from beef heart, it is not a
specific test. This test is also classified as non-specific or non-treponemal or standard test. The antibodies reacting
with cardiolipin antibodies have been traditionally (but incorrectly) termed “regain”.

Principle: Patients suffering from syphilis produce antibodies that react with cardiolipin antigen in a slide
flocculation test, which are read using a microscope. It is not known if the antibodies that react with cardiolipin are
produced against some lipid component of Treponema pallidum or as a result of tissue injury following infection.

Requirements: Patient’s serum, water bath, freshly prepared cardiolipin antigen, VDRL slide, mechanical rotator,
pipettes, hypodermic syringe with unbeveled needle and microscope. Known reactive and non-reactive serum
controls are also required.

VDRL antigen: The cardiolipin antigen is an alcoholic solution composed of 0.03% cardiolipin, 0.21% lecithin and
0.9% cholesterol. The cardiolipin antigen must be freshly constituted each day of test. The working antigen is a
buffered saline suspension of cardiolipin.

VDRL slide: This is a glass slide measuring 2 X 3 inch with 12 concave depressions, each measuring 16 mm in
diameter and 1.75 mm deep.

Procedure: Patients’ serum is inactivated by heating at 56o
C for 30 minutes in a water bath to remove non-specific
inhibitors (such as complement). The test can be performed both qualitatively and quantitatively. Those tests that
are reactive by qualitative test are subjected to quantitative test to determine the antibody titres.

Qualitative test: 0.05 ml of inactivated serum is taken into one well. 1/60th ml (or 1 drop from 18 gauge needle) of
the cardiolipin antigen is then added with the help of a syringe (unbeveled) to the well and rotated at 180 rpm for 4
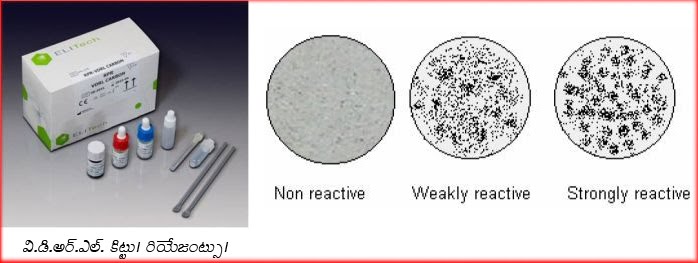
minutes. Every test must be accompanied with known reactive and non-reactive controls. The slide is then viewed
under low power objective of a microscope for flocculation. The reactive and non-reactive controls are looked first to
verify the quality of the antigen. Depending on the size the results are graded as weakly reactive (W) or reactive
(R). Reactive samples are then subjected to quantitative test.
Qualitative test: this is performed to determine the antibody titres. The serum is doubly diluted in saline from 1in 2
to 1:256 or more. 0.05 ml of each dilution is taken in the well and 1/60 ml of antigen is added to each dilution and
rotated in a rotator. The results are then checked under the microscope. The highest dilution showing flocculation is
considered as reactive titre. Sometimes, due to very high level of antibodies in the serum (prozone phenomenon)
the qualitative test may be non-reactive. If the clinical findings are strongly suggestive of syphilis, a quantitative test
may be directly performed on the serum specimen.

CSF VDRL: VDRL test may also be performed on CSF samples in the diagnosis of neurosyphilis. Quantitative
VDRL is the test of choice on CSF specimens. However, there are some variations in this test. The antigen is
diluted in equal volumes with 10% saline, CSF must not be heated (or inactivated), the volume of antigen solution
taken is 0.01 ml (or 1 drop from 21 gauge needle) and rotation time is 8 minutes. Rest of the procedure remains
same.



Significance of VDRL test: VDRL test becomes positive 1-2 weeks after appearance of (primary lesion) chancre.
The test becomes reactive (50-75%) in the late phase of primary syphilis, becomes highly reactive (100%) in the
secondary syphilis and reactivity decreases (75%) thereafter. Treatment in the early stages of infection may
completely suppress production of antibodies and result in non-reactive tests. Effective treatment in the primary or
secondary stages results in rapid fall in titre and the test may turn non-reactive in few months. Treatment in latent or
late syphilis has very little effect on the titre and the titres may persist at low levels for long periods. Since the titre
falls with effective treatment, it can be used for assessment of prognosis. VDRL test is more suitable as a screening
agent than a diagnostic tool.
VDRL test is also helpful in the diagnosis of congenital syphilis. Since passively transferred antibodies through
placenta may give false reactive test in serum of the infant, a repeat test after a month showing no increase in titre
may help rule out congenital syphilis.
Since the test employs a non-treponemal antigen, there are many chances of false positive results. False positivity
(other than technical) may be due to physiological of pathological conditions. These are called biological false
positives (BFP). If the remain positive for less than 6 months it is considered acute and they remain positive for
longer than 6 months it is called chronic BFP. The physiological reasons for BFP include pregnancy, menstruation,
repeated blood loss, vaccination, severe trauma etc while the reasons for pathological BFP include malaria,
infectious mononucleosis, hepatitis, relapsing fever, tropical eosinophilia, lepromatous leprosy, SLE, rheumatoid
arthritis etc.
A reactive VDRL test does not necessarily imply that the person is syphilitic. The diagnosis must be made in
conjunction with clinical findings. Any reactive VDRL test must be confirmed with a specific or treponemal test such
as TPHA, FTA-ABS test.

INSTAGRAM


Hiç yorum yok:
Yorum Gönder